
.svg)
.svg)


What Is Buerger’s Disease and How Does It Damage Circulation?
Buerger’s disease, also known as thromboangiitis obliterans, is an inflammatory condition that damages small and medium-sized blood vessels. Most commonly, it impacts the arms and legs and is strongly linked to tobacco exposure. As blood vessels become inflamed and blocked, tissues receive less oxygen, which raises the risk of pain, wounds, and tissue loss.
This condition differs from common peripheral artery disease caused by plaque buildup. Buerger’s disease typically affects younger adults and often progresses in a different vascular pattern. That distinction matters because treatment priorities focus less on plaque control and more on removing the underlying trigger while protecting tissues that can still heal.
Buerger’s Disease Causes and Risk Factors

Tobacco exposure is the primary trigger. Chemicals in nicotine products damage blood vessel linings and initiate inflammation. This process leads to clot formation and reduced circulation.
- Immune response: Abnormal inflammatory reactions within blood vessels.
- Genetic susceptibility: Increased likelihood in certain populations.
- Chronic irritation: Repeated exposure to harmful substances in tobacco.
Although multiple factors may contribute, removing tobacco exposure continues to be the most effective way to limit further damage. The National Institutes of Health Buerger’s disease clinical review shows that continued tobacco use plays a central role in both disease progression and the risk of limb loss in Buerger’s disease patients. Without that step, other treatments won’t be as impactful.
Symptoms of Buerger’s Disease
Symptoms often develop gradually and may initially resemble other vascular conditions. Pain during walking or activity is a common early sign. As the disease progresses, symptoms may occur even at rest.
- Pain in extremities: Discomfort in feet, toes, hands, or fingers during activity or rest.
- Skin discoloration: Pale, bluish, or reddish changes indicating poor circulation.
- Cold sensitivity: Increased discomfort in low temperatures.
- Ulcers: Non-healing sores on fingers or toes.
- Numbness or tingling: Reduced sensation caused by impaired blood flow.
- Burning sensation: Nerve irritation linked to ischemia.
- Early gangrene: Tissue breakdown in advanced stages.
Don’t ignore these signs, especially in individuals with a history of tobacco use. Early evaluation allows for intervention before tissue damage becomes irreversible.
How Buerger’s Disease Is Diagnosed
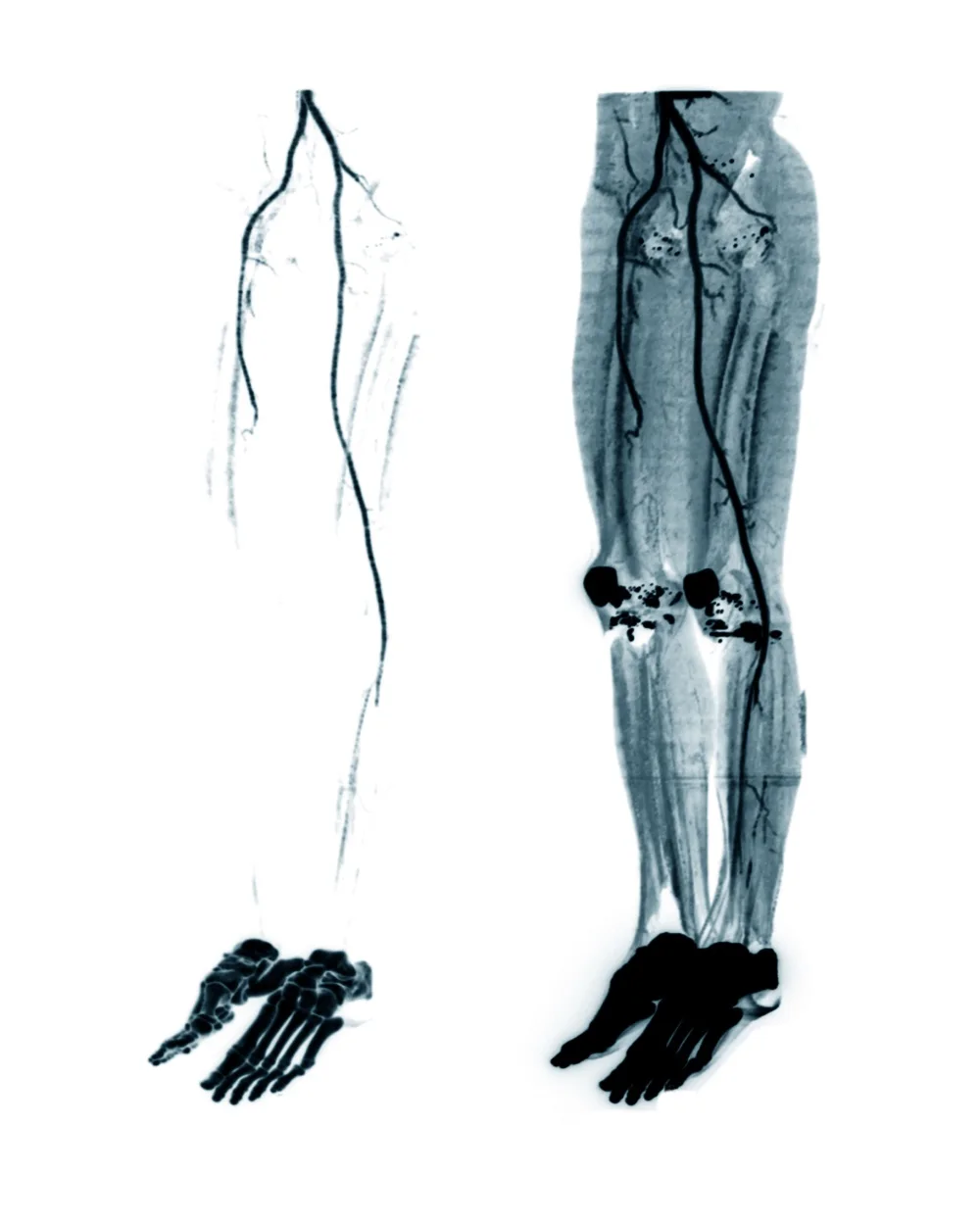
Diagnosis is primarily clinical and involves ruling out other vascular conditions, such as atherosclerosis or autoimmune diseases. Physicians assess medical history, particularly tobacco use, and perform physical examinations focusing on blood flow and tissue condition. Imaging studies, including angiography, may reveal characteristic patterns of vessel blockage.
Laboratory tests are often used to exclude other causes of vascular inflammation. Accurate diagnosis allows for appropriate management strategies, which are essential for preventing irreversible damage. Early intervention is critical to preserve limb integrity.
Medical Treatment for Buerger’s Disease

Medical care focuses on symptom control and tissue preservation. Treatment varies depending on disease severity and extent of damage.
- Pain management: Medications to reduce discomfort and improve quality of life.
- Circulation support: Drugs that promote blood flow in affected areas.
- Wound care: Treatment of ulcers to prevent infection and promote healing.
- Antibiotic therapy: Infection control in open wounds.
- Monitoring: Regular follow-up to track disease progression.
- Environmental protection: Avoidance of cold exposure and physical trauma.
These measures are designed to slow disease progression and protect viable tissue, with effectiveness heavily dependent on early implementation and patient adherence.
How Buerger’s Disease Progresses to Amputation
Buerger’s disease typically advances in stages as blood flow to the extremities becomes increasingly restricted. What may start as mild discomfort or sensitivity can gradually develop into tissue damage when circulation is no longer sufficient to support healing. If intervention is delayed or the disease continues to progress, it may be necessary to remove the affected tissue surgically.
The progression often follows a recognizable pattern:
- Reduced blood flow: Inflammation and clot formation limit circulation to the fingers or toes, leading to pain and cold sensitivity.
- Persistent ischemic pain: Discomfort may begin during activity and progress to constant pain at rest as oxygen supply decreases.
- Non-healing ulcers: Minor injuries or pressure points develop into wounds that do not heal due to inadequate blood flow.
- Infection development: Open sores increase the risk of infection, which can spread and worsen tissue damage.
- Gangrene formation: Severely compromised tissue begins to die, often appearing dark or blackened.
- Functional loss: The affected area can no longer support movement or weight-bearing, limiting mobility.
At this stage, amputation may be needed to remove nonviable tissue and prevent further complications. Surgical planning prioritizes preserving limb length while selecting a level that will heal reliably and support effective prosthetic use.
Rehabilitation After Buerger’s Disease Amputation
Rehabilitation begins shortly after surgery and involves a multidisciplinary approach. Physical therapy focuses on strengthening, balance, and mobility training. Patients are also educated on residual limb care to prevent complications such as skin breakdown or infection.
Psychological support is often helpful in addressing the emotional impact of limb loss. A structured rehabilitation program improves functional outcomes and prepares individuals for prosthetic fitting. Early engagement in rehabilitation contributes to better long-term mobility and independence.
Prosthetic Solutions for Buerger’s Disease Patients

The ideal prosthetic depends on the level of amputation, activity level, and individual goals. Each option should balance mobility, stability, and tissue tolerance, especially if circulation has been compromised.
Below-Knee Prosthetics
Below-knee prosthetics are commonly used when the knee joint is preserved. This allows for more natural movement patterns and reduces the energy required for walking. Many systems include energy-storing prosthetic feet that improve efficiency and support smoother gait transitions.
Above-Knee Prosthetics
Above-knee prosthetics require more advanced components because they replace the natural knee joint. Microprocessor-controlled knees are often used to adapt to walking speed and terrain in real time. These systems improve stability and help reduce the risk of falls during daily activities.
Socket Technology and Direct Socket Systems
Custom socket design plays a central role in both comfort and function. The socket serves as the connection between the residual limb and the prosthesis, so proper fit is essential for long-term use. Direct socket systems mold directly to the limb, enabling faster fabrication, improved comfort, and reduced fitting time.
Upper Extremity Prosthetics
Upper extremity prosthetics may be considered in cases where the disease affects the hands. These devices range from cosmetic solutions to functional systems that restore grasp and controlled movement. The specific prosthetic depends on the level of limb loss and the patient’s functional goals.
Role of Orthotics in Early and Mid-Stage Disease
Orthotic devices may be used before amputation becomes necessary. Custom foot orthotics can help redistribute pressure and reduce the risk of ulcer formation. Ankle-foot orthoses (AFOs) may provide additional support and improve gait in patients with compromised circulation.
These devices help limb preservation by minimizing mechanical stress on vulnerable tissues. Regular adjustments are necessary to accommodate changes in the patient’s condition. Orthotic management is often integrated into a broader treatment plan focused on maintaining mobility.
Managing Buerger’s Disease and Moving Toward Recovery
Stopping tobacco usage is the pivotal factor in the progression of Buerger’s disease. Patients who eliminate nicotine exposure often experience stabilization, while continued use leads to worsening symptoms and a higher risk of amputation. Ongoing medical supervision plays a key role in monitoring vascular health and managing complications.
Long-term care includes regular follow-up visits, prosthetic maintenance, and lifestyle modifications. Advances in prosthetic technology continue to improve mobility and quality of life for individuals who undergo amputation. With appropriate management, many patients achieve functional independence and return to daily activities.